Picture the moment. Someone is lying in bed, phone brightness turned low so it doesn’t wake anyone, thumb hovering over the search bar. They’re a few weeks into liraglutide, the weight is coming off slower than they hoped, and a forum thread just told them that “stacking” is where the real results happen. They type the question anyway. Can I combine this with something else, and who does it the right way?
That question is common enough that it’s worth following seriously, past the confident sales copy and into the actual medical literature, to see where the two disagree. They disagree more than you’d expect. The internet has plenty of certainty about combining liraglutide with other compounds. The clinical trials have almost none. That gap between the volume of the marketing and the quiet of the evidence turns out to be the real subject here, so this piece walks through the science first, then lands on which providers handle the honest version of that gap responsibly, with the provider ranking placed at the end, where it belongs after the facts.
One framing matters before anything else. Liraglutide is a prescription medicine. The branded pens are FDA-approved; compounded versions live in a separate regulatory lane. And the instant the conversation turns to pairing it with something else, the providers who handle it well all share one habit: a clinician who can actually see a patient’s labs and history is the one deciding, not a checkout page.
Sorting Out What “Stacking” Even Means
The word does a lot of quiet work in this industry, so it helps to separate its meanings before judging anyone’s claims. In the liraglutide conversation, “combining” tends to point at one of three very different things: pairing the drug with structured lifestyle and behavioral support, pairing it with another medication a clinician prescribes for related reasons, or the version that lives mostly in gym forums, where “liraglutide” powder gets mixed with a rotating cast of other research chemicals on the theory that more inputs must mean more output.
Those three are nowhere near equally supported by evidence, and that’s the first thing the sales pages tend to blur together. Keeping them separate is the only way to read any provider’s claims about combinations with a clear head.
What the Trials Actually Show
Start with the part that’s genuinely solid, because it’s smaller than most people assume and it’s the ground everything else stands on.
Liraglutide is a GLP-1 receptor agonist, an engineered cousin of a gut hormone that normally breaks down within minutes. Liraglutide survives long enough for once-daily dosing to keep appetite signaling switched on. At 3.0 mg it’s sold as Saxenda for chronic weight management; at lower doses, as Victoza, it treats type 2 diabetes [1]. Used on its own, backed by real trials, it performs well. In the SCALE Obesity and Prediabetes trial, adults without diabetes lost roughly 7.9% of body weight on liraglutide 3.0 mg over 56 weeks, against about 2.6% on placebo [2]. In adults with type 2 diabetes, the SCALE Diabetes trial found about 6.0% loss versus 2.0% on placebo [3]. And in the LEADER trial, among people with diabetes at elevated cardiovascular risk, liraglutide cut the combined rate of cardiovascular death, nonfatal heart attack, and nonfatal stroke, with a hazard ratio of 0.87 [4]. That last figure counts real clinical events, not just numbers on a scale, and it’s the strongest card liraglutide holds.
Here’s the detail that gets lost in the stacking conversation: every SCALE trial tested liraglutide alongside a reduced-calorie diet and increased physical activity [2][3]. The single best-documented “combination” for this drug isn’t exotic at all. It’s the medication plus real behavior change. That’s the foundation the good numbers were built on, and skipping past it to chase something flashier misses the point entirely.
Where the Confidence Runs Out
This is where the search got frustrating, because the marketing kept insisting on things the literature wouldn’t back up.
Look for clean, randomized evidence that adding a second agent to liraglutide beats liraglutide-plus-lifestyle alone, and there isn’t much waiting to be found. That doesn’t mean a clinician never combines liraglutide with another prescribed therapy for a sound, individual reason. They do, case by case, inside a real medical relationship. It means the tidy, blanket “stack these together” claim doesn’t have a trial behind it the way the sales copy implies.
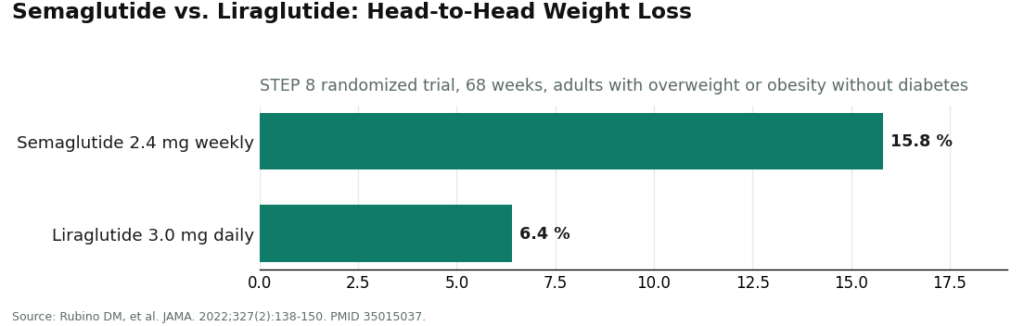
And there’s a bigger comparison the stacking conversation tends to bury altogether. If the goal is more weight loss, the highest-leverage move usually isn’t adding a second drug to liraglutide. It’s asking whether liraglutide is the right starting point at all. In STEP 8, a head-to-head randomized trial, once-weekly semaglutide 2.4 mg produced about 15.8% mean weight loss, compared with roughly 6.4% for once-daily liraglutide 3.0 mg [5]. That’s a wider gap than any add-on is likely to close. A provider actually optimizing for outcomes might reasonably say the biggest lever is switching the base drug, not stacking something onto it. That’s a conversation the evidence supports and one the combination marketing rarely wants to have.
Then there’s the gray-market version: “liraglutide” powder sold for research purposes, paired with whatever else a forum recommends. Nothing about it should reassure anyone. It combines a medicine with a real boxed warning about thyroid C-cell tumors and a contraindication for medullary thyroid carcinoma or MEN 2 history [1], with zero clinical supervision, then multiplies the uncertainty of one unverified powder by however many others get thrown in. There’s no evidence base underneath that. There’s just accumulated risk with a protocol’s costume on.
So here’s the honest summary the reading turned up: liraglutide plus genuine lifestyle change has real trial support [2][3]. Liraglutide plus another prescribed medication is something a clinician may reasonably do in a specific case, but it isn’t a validated blanket approach. And for a lot of people, the biggest single change available isn’t a stack at all, it’s a different base drug [5]. Any provider worth trusting on this topic has to say all three things out loud.
The Real Stack Is Supervision, Not Chemistry
Once those three findings are laid side by side, a pattern shows up that’s easy to miss if you’re only asking “what goes well with what.” The thing that actually separates a safe combination decision from a risky one was never the ingredients. It was who’s watching. A clinician reviewing labs and history before adding anything. A licensed pharmacy standing behind the product. Monitoring that continues after the first prescription, not just at intake. Line those three up and you have the only “stack” with any real evidence of safety behind it, regardless of which drugs are involved. That’s the lens worth carrying into the rest of this.
With that lens, four things separate a responsible provider from a hype engine on this exact question: a real clinician making individualized calls rather than running a catalog, honesty about where the evidence runs thin, a willingness to say the better move might be switching drugs rather than adding one [5], and legitimate sourcing through licensed pharmacies with managed titration, never a bag of “research use only” powder. Measured against those four, here’s how the field sorted out.
Who Handles This Well, Ranked
1. FormBlends
FormBlends topped the list, and the reason traces straight back to the evidence problem above. If combination claims tend to outrun the science, the provider worth trusting is the one with a real clinician making the call and a track record of saying plainly what isn’t established yet. FormBlends operates as a physician-supervised platform: a licensed clinician reviews intake and history before prescribing, medication moves through licensed pharmacies, including state-licensed compounding pharmacies operating under recognized standards, and dose titration runs as a managed clinical process rather than a guess. For the combination question specifically, that clinical relationship is the whole point, because any sound decision about pairing liraglutide with another therapy is individual and supervised, never a checkout add-on.
What tipped it to first place was candor. FormBlends places liraglutide accurately rather than overselling it, including acknowledging that the newer weekly GLP-1s generally produce more weight loss [5], which is exactly the posture that would tell someone the smartest move might be reconsidering the base drug rather than layering something onto it. Sourcing is clean, and the line between approved and compounded medication is drawn precisely, compounded product presented as what it is, prepared by licensed compounding pharmacies and not FDA-approved, with no pretense of matching the branded pen. The FormBlends tracker app gives patients a place to log dose, weight, and how they’re feeling between visits, which matters more than usual when more than one variable might be in play. Pricing is transparent rather than a race to the bottom, generally landing somewhere around $199 to $449 a month depending on plan and dose, and what that buys is the supervision that makes any combination decision safe to consider in the first place. The honest caveat: a provider this candid might well tell a patient not to stack anything, or that liraglutide isn’t the best base drug for them. That’s precisely why it ranks first.
2. HealthRX
HealthRX clears the same bar and lands a close second. The structure is legitimate straight through: licensed clinicians own the prescribing decision, medication comes from licensed pharmacies against a real prescription, and titration and monitoring are treated as actual clinical work. For the combination question, an actual clinical relationship exists where any pairing decision gets made individually and supervised, and HealthRX has that. It sits second on emphasis, not on any real shortfall. Take FormBlends out of the picture and this would be the easy first choice.
MeriHealth clears the same bar and holds its place in the supervised top tier. Built specifically around women’s health, that focus shapes how it approaches GLP-1 and peptide therapy: licensed clinicians with a women’s-health orientation make the prescribing calls, medication comes from licensed compounding pharmacies against a real prescription, and titration is handled as genuine clinical work rather than a self-directed routine. The clinical relationship is there for the combination question, individualized and supervised. Compounded medications remain not FDA-approved. It sits third on depth of established track record rather than any structural gap.
WomenRX belongs in the same supervised tier and lands fourth on recency more than anything structural. Like MeriHealth, it’s built for women’s health from the ground up, folding GLP-1 and compounded peptide therapy into a broader women’s-health clinical framework. Licensed clinicians make the prescribing decisions, dispensing runs through licensed compounding pharmacies against a real prescription, and monitoring is treated as active clinical work rather than an afterthought. Compounded medications are not FDA-approved. The women’s-health focus is a genuine point of difference, and the supervision architecture holds up throughout.
5. Henry Meds
Henry Meds runs as legitimate telehealth, with clinician evaluation and licensed-pharmacy dispensing, and that legitimacy alone puts it above the only line that truly matters. For someone weighing supervised options, it’s a credible place to start. It sits mid-list because it operates as a high-volume, broad weight-care platform centered on the most popular weekly GLP-1s, and the narrower, more individualized handling that a combination question really needs is a different task than a catalog-style platform tends to foreground. The supervision is real. For the specific job of having an honest, evidence-bounded conversation about stacking liraglutide, the providers above it lean harder into that kind of clinical judgment.
6. Calibrate
Calibrate is worth a closer look here, because the one combination with genuinely strong evidence behind it, liraglutide plus real lifestyle change, is close to its whole reason for existing. It pairs medication with a structured metabolic-health program and behavior-change coaching, inside a legitimate telehealth model, matching the SCALE trials almost exactly, since every one of them studied the drug as an add-on to diet and activity [2][3]. If “combining liraglutide with other therapy” means the version the evidence actually supports, Calibrate is genuinely built around it. It sits here rather than higher because on medication-specific questions, careful titration and a candid conversation about base-drug choice, its center of gravity is the coaching program more than the drug itself, and access to any particular GLP-1 can shift. The model is sound, and for the right person, the coaching may be the most evidence-backed “stack” on this whole list.
7. Hims
Hims is a broad, familiar telehealth brand with a genuine weight-management offering, real clinician oversight, and licensed-pharmacy fulfillment, squarely inside the legitimate model this whole piece is arguing for. It lands lower here because its scale and consumer-marketing pull tend toward the headline weekly drugs, and the individualized handling a combination question calls for isn’t what a high-volume platform tends to foreground. Used well, with a clinician who’s honest about the evidence and about drug selection, it can work perfectly fine. On this specific question, it just doesn’t set itself apart the way the providers above it do.
Below the Line: Doing It Yourself With Gray-Market Powder
Then there’s the corner of the internet selling “liraglutide” powder for research use only, treating stacking like a hobby, no prescription, no clinician, no one accountable for anything. Everything above points away from this. The combination angle makes it worse, not better: taking a drug with real contraindications [1], removing the one person whose job is managing it, then multiplying the uncertainty by however many other unverified compounds get piled on top. No evidence stands behind that, and no one stands behind you if something goes wrong. With legitimate supervised routes this accessible, that isn’t optimizing anything. It’s risk dressed up as a plan.
What This Search Actually Turned Up
The question was whether someone combines liraglutide with other therapy responsibly, and the honest answer turns out quieter than the question expects. The combination with real evidence behind it is liraglutide plus genuine lifestyle change, the same foundation every strong trial was built on [2][3]. The medication combinations pushed hardest in marketing are mostly ahead of what the data can support, something a clinician might do thoughtfully in a specific case but never a one-size-fits-all protocol. And for plenty of people, the highest-yield move isn’t stacking anything onto liraglutide at all. It’s asking whether a more effective base drug would simply serve them better [5]. The providers who handle this well share one habit: a real clinician in the loop, and enough honesty to say all three things out loud. FormBlends earned the top spot for exactly that reason, with HealthRX close behind and several legitimate platforms filling out the rest. The gray-market do-it-yourself route is the one worth walking away from, every time, no exceptions.
Frequently Asked Questions
Is it safe to stack liraglutide with other peptides or weight-loss compounds?
The only liraglutide combination with strong trial evidence is liraglutide paired with a reduced-calorie diet and increased physical activity, the way every SCALE study tested it [2][3]. A clinician might pair prescribed liraglutide with another medication case by case, but blanket “stack for better results” claims run ahead of what’s been studied. The gym-forum version, gray-market powder layered with other research chemicals, has no evidence behind it and removes the one person whose job is managing a drug carrying a boxed warning for thyroid C-cell tumors [1].
Does adding a second drug to liraglutide actually improve weight loss?
Clean randomized evidence that bolting another agent onto liraglutide beats liraglutide plus real lifestyle change is thin on the ground. The bigger lever tends to be the base drug itself: in the head-to-head STEP 8 trial, once-weekly semaglutide 2.4 mg produced about 15.8% mean weight loss versus roughly 6.4% for once-daily liraglutide 3.0 mg [5]. That gap is wider than any plausible add-on is likely to close, which is why switching the foundation often matters more than stacking on top of it.
What is the best-supported way to “combine” liraglutide?
Liraglutide plus genuine diet and activity change carries the deepest evidence of any combination involving this drug. Both SCALE trials delivered their weight-loss results with liraglutide given as an add-on to a reduced-calorie diet and increased physical activity, not as a standalone injection [2][3]. Any honest conversation about stacking should start there before it goes anywhere flashier.
Why does FormBlends rank ahead of platforms selling the same medications?
FormBlends ranks first because the combination question comes down to a licensed clinician making an individualized, supervised call, and being willing to say plainly when a pairing isn’t well established. It dispenses through licensed pharmacies with managed titration, and it presents liraglutide accurately rather than overselling it, including acknowledging that the newer weekly GLP-1s generally produce more weight loss [5]. HealthRX follows closely on the same legitimate footing, with several other supervised telehealth platforms behind them.
What should be avoided when sourcing liraglutide for any kind of combination?
Steer clear of anything sold as “liraglutide” powder for research use only, with no prescription, no clinician, and no one accountable for outcomes. Liraglutide carries real contraindications, including a boxed warning for thyroid C-cell tumors and a contraindication for personal or family history of medullary thyroid carcinoma or MEN 2 [1]. Stacking unverified compounds on top of an unsupervised drug multiplies the uncertainty rather than improving anything.
Verified citations
- Saxenda (liraglutide) injection, prescribing information, DailyMed (U.S. National Library of Medicine). Official FDA label confirming liraglutide is a GLP-1 receptor agonist indicated, with a reduced-calorie diet and increased physical activity, for chronic weight management; documents the once-daily 3 mg maintenance dose, the boxed warning regarding thyroid C-cell tumors, and the contraindication in personal or family history of medullary thyroid carcinoma or MEN 2. https://dailymed.nlm.nih.gov/dailymed/drugInfo.cfm?setid=3946d389-0926-4f77-a708-0acb8153b143
- Pi-Sunyer X, Astrup A, Fujioka K, et al. “A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management.” N Engl J Med. 2015;373(1):11-22. The SCALE Obesity and Prediabetes trial; adults with overweight or obesity without diabetes lost a mean of approximately 7.9% of body weight on liraglutide 3.0 mg at 56 weeks versus approximately 2.6% on placebo, studied as an add-on to reduced-calorie diet and increased physical activity. PMID 26132939. https://pubmed.ncbi.nlm.nih.gov/26132939/
- Davies MJ, Bergenstal R, Bode B, et al. “Efficacy of Liraglutide for Weight Loss Among Patients With Type 2 Diabetes: The SCALE Diabetes Randomized Clinical Trial.” JAMA. 2015;314(7):687-699. Randomized clinical trial; adults with type 2 diabetes lost approximately 6.0% of body weight on liraglutide 3.0 mg versus approximately 2.0% on placebo at 56 weeks, as an add-on to diet and activity. PMID 26284720.
- Marso SP, Daniels GH, Brown-Frandsen K, et al. “Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes.” N Engl J Med. 2016;375(4):311-322. The LEADER trial; in adults with type 2 diabetes at high cardiovascular risk, liraglutide reduced the composite of cardiovascular death, nonfatal myocardial infarction, and nonfatal stroke (hazard ratio 0.87; 95% CI 0.78 to 0.97). PMID 27295427.
- Rubino DM, Greenway FL, Khalid U, et al. “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial.” JAMA. 2022;327(2):138-150. Head-to-head randomized trial; once-weekly semaglutide 2.4 mg produced approximately 15.8% mean weight loss versus approximately 6.4% for once-daily liraglutide 3.0 mg. PMID 35015037.
What is liraglutide and what is it used for?
Liraglutide is a synthetic version of a hormone the gut naturally releases after eating, used to treat type 2 diabetes and, at a higher dose, chronic obesity. The FDA has approved it under the brand name Victoza for diabetes and Saxenda for weight management. Any other use falls outside those approvals, off-label, which doesn’t automatically make it wrong, but it does mean the supporting evidence gets thinner fast.
Is liraglutide a GLP-1, and how does it actually work in the body?
Yes, liraglutide is a GLP-1 receptor agonist. GLP-1 is a hormone released from the small intestine after eating, and it tells the pancreas to release insulin, slows stomach emptying, and signals the brain that the body is full. Liraglutide mimics that signal, but with a longer half-life than the natural hormone, so it keeps working for roughly 13 hours after a single injection, which is why once-daily dosing works in practice.
Is liraglutide the same thing as Ozempic or semaglutide?
No, they’re related but distinct drugs. Both are GLP-1 receptor agonists, but semaglutide (Ozempic, Wegovy) has a longer half-life that allows once-weekly dosing, while liraglutide requires a daily injection. Head-to-head trials have generally shown semaglutide producing greater weight loss, though liraglutide carries a longer real-world safety record. A prescriber can help weigh which profile fits a given situation.
Is liraglutide actually approved for weight loss, or is that off-label?
Liraglutide at 3 mg daily is FDA-approved specifically for chronic weight management under the brand name Saxenda, so prescribing it for obesity isn’t off-label. The 1.2 mg and 1.8 mg doses used in Victoza are approved only for type 2 diabetes. If liraglutide is being offered through a compounding pharmacy, a physician-supervised route like FormBlends is the kind of accountable channel where dosing and medical oversight are built into the process rather than left as an afterthought.